Clinical assessments in psychiatric practice mostly rely on verbal report of symptoms by individuals who experience them. Some of these self- reports are corroborated by family members or other associates, providing information required to formulate the problem that needs attention.
Another important source of information is the observed behaviour.
Both motor and language behaviour are relevant in this regard.
In medical practice, self-reported phenomena are called symptoms, while observed (not reported) features are called signs. Signs are generally elicited by performing certain manoeuvres.
In psychiatry, such manoeuvring is not practiced often. The closest we come to is posing questions in a certain way to elicit the self-endorsed symptom we are looking for (e.g. graded questioning to elicit suicidal ideas).
Cognitive tests can be seen as one form of testing or manoeuvring to elicit certain signs. But most cognitive tests do not provide sufficiently specific information that allows clinical actions to follow.
The study of language behaviours and motor behaviours in more systematic fashion, e.g. by recording speech samples or using video analyses of expressions may provide us means to establish the subtle psychiatric signs that are missing in our practice at present.
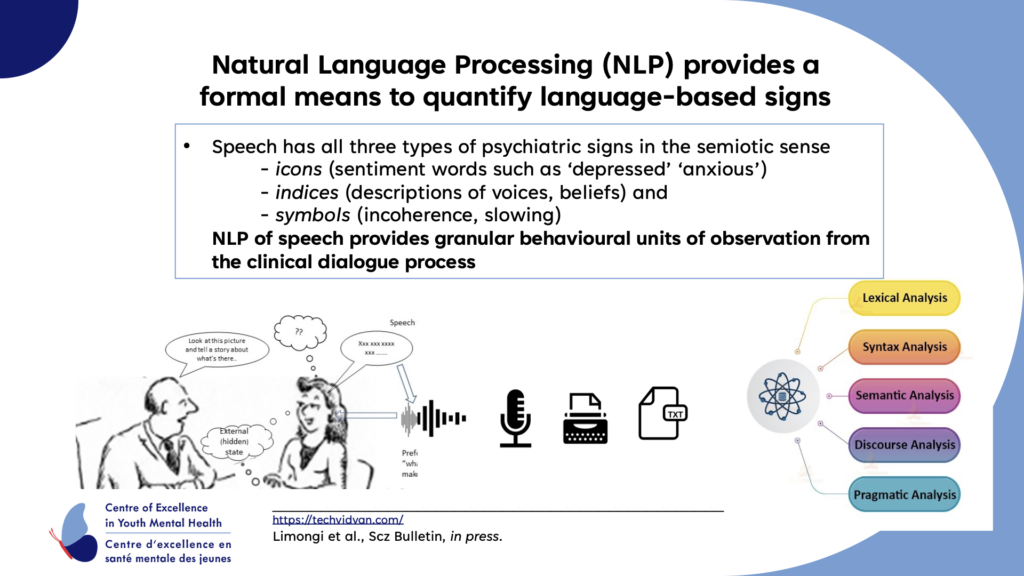
Speech in particular carries the full spectrum of semiotic tools (i.e. signs that communicate a meaning that is other than the sign itself). Using Natural Language Processing (NLP) may provide a way for us to scale up the study of these signs, and distill them for clinical use.